Are you struggling with persistent knee pain and a feeling of instability after an unexpected blow or sports injury? If you suspect a problem deeper than a typical sprain, you may be dealing with a PCL injury.
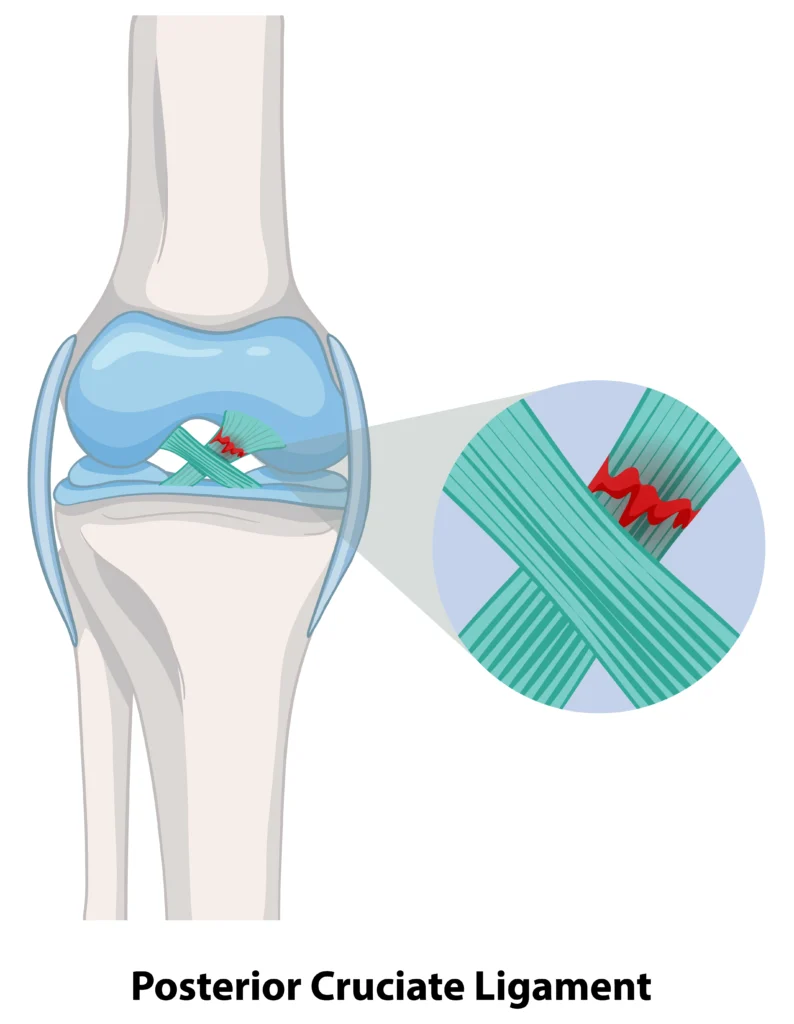
A PCL injury occurs when the strong ligament at the back of the knee is subjected to excessive force. The PCL is a vital band of tissue that prevents the shinbone (tibia) from moving too far backward relative to the thighbone (femur). Understanding the mechanism of injury is crucial for both prevention and accurate diagnosis.
The most common cause of a PCL injury is a direct blow to the front of the shin whilst the knee is bent at 90 degrees. This classic mechanism earned the nickname “dashboard injury” because it frequently occurs during motor vehicle accidents when the knee strikes the dashboard.
Sports-related PCL tears often happen when an athlete falls onto a bent knee with the foot pointed downward—common in football, rugby, and basketball. The ground drives the tibia backwards, overstretching or tearing the PCL. This same mechanism can occur during motorcycle accidents or any situation where direct force is applied to the proximal tibia.
Hyperextension injuries occur when the knee is forced to straighten beyond its normal limit. This mechanism can tear the PCL, often alongside other knee ligaments including the ACL, MCL (medial collateral ligament), or LCL (lateral collateral ligament).
Multi-ligament knee injuries are particularly serious. They typically result from high-energy trauma such as:
When multiple ligaments are torn simultaneously, the knee becomes severely unstable and almost always requires surgical reconstruction by an experienced orthopaedic surgeon.
PCL injuries are graded based on the severity of the damage, which directly influences the appropriate treatment. We use a clear classification system:
The distinction between a partial PCL tear and a complete tear is the most important factor in deciding between non-surgical care and PCL reconstruction surgery.
Recognising the symptoms of a torn PCL ligament can be difficult because the initial pain and swelling are often less severe than with an ACL tear. However, the unique function of the PCL means its injury presents specific, tell-tale signs of instability. This section details the symptoms to look for, helping you differentiate this injury from other knee problems.
Unlike some other knee injuries, the pain from a PCL tear is typically localised and may not feel immediately debilitating. Key symptoms often include:
If you are experiencing a feeling of instability that affects your daily movement, consulting with a specialist like Dr Ren is essential for an accurate assessment.
Understanding the differences between ACL and PCL injuries helps with accurate self-assessment before seeing a knee pain specialist:
| Symptom Feature | ACL Tear | PCL Tear |
|---|---|---|
|
Initial “Pop” |
Often heard or felt; distinct. |
Less common or subtle. |
|
Swelling |
Often rapid and severe (within hours). |
Usually less severe and develops gradually. |
|
Instability |
The knee “gives out” forward/sideways. |
The knee feels unstable with a backward sag. |
|
Location of Main Pain |
Front of the knee/joint line. |
Back of the knee; front of the knee when kneeling. |
An ACL vs. PCL MRI scan can definitively distinguish between these injuries. MRI imaging reveals the specific ligament damage, tear location, and any associated injuries to menisci or other structures.
Achieving a good long-term outcome for a posterior cruciate ligament tear begins with precise diagnosis and grading. At TOPP, Dr Ren uses a systematic approach, combining expert physical examination with precision imaging to accurately determine the extent of the damage and classify the grading for PCL injuries.
A definitive diagnosis often starts in the clinic with a specialised physical examination. The key diagnostic technique for a PCL tear is the posterior drawer test.
During this PCL injury test, the patient lies on their back with the knee bent at a 90-degree angle. Dr Yong Ren will gently push the upper part of the shinbone backward. If the PCL is torn, the shinbone will move backward excessively or “sag,” indicating laxity in the joint. This test is crucial for assessing the degree of posterior instability. Other tests, such as checking for the ‘posterior sag sign’ while the knee is at rest, further help confirm the diagnosis.
While the physical exam provides strong evidence, imaging is indispensable for confirming the extent of the posterior cruciate ligament tear and checking for co-existing injuries.
Accurate grading ensures that the treatment plan (whether conservative or surgical) is perfectly matched to the severity of your unique PCL injury.
The PCL possesses a better capacity for natural healing than the ACL, meaning that many isolated PCL injuries, particularly Grade I and Grade II partial PCL tear cases, can be managed effectively without surgery. The non-surgical approach is centred on reducing initial symptoms and meticulously strengthening the surrounding muscles to restore knee stability.
Immediate management following a PCL injury center on the R.I.C.E. protocol:
A knee brace for PCL injury plays a crucial role in conservative treatment. Functional knee braces are designed to prevent the tibia from sagging backward, which could stress the healing ligament. Your orthopaedic doctor may recommend wearing this brace for 4-6 weeks during the initial healing phase and during rehabilitation activities.
Physiotherapy is the most critical element of non-surgical recovery. A structured rehabilitation program may be designed to compensate for the damaged PCL by maximising surrounding muscle strength and control.
The Quadriceps Focus: The PCL’s primary antagonist is the quadriceps muscle group (front of the thigh). Strengthening the quadriceps actively pulls the shinbone forward, counteracting the posterior sag and providing a dynamic stabilising force that protects the PCL.
Key Rehabilitation Strategies:
It is equally important to know the PCL injury exercises to avoid in the initial phases, such as open-chain hamstring curls, which can place undue stress on the healing PCL by pulling the shinbone backward.
Whilst most PCL injuries heal without surgery, certain situations require surgical reconstruction. Surgery becomes necessary when conservative treatment fails to restore adequate knee stability or when the injury severity makes non-surgical healing unlikely. The decision involves careful consideration of your activity level, symptoms, and associated injuries.
Surgery is less common for an isolated PCL tear than for an ACL tear, but it is necessary in cases where the knee is significantly unstable. The decision for PCL reconstruction is typically based on the following criteria:
For athletes or individuals with physically demanding occupations, surgery may be considered earlier to ensure a robust return to high-impact activities.
PCL reconstruction involves replacing the torn ligament with a tissue graft, which may be sourced from the patient’s own body (autograft) or a donor (allograft).
Orthopaedic surgeons perform this procedure using an arthroscopic (minimally invasive) technique. This involves inserting a small camera and instruments through tiny incisions around the knee. The benefits of this approach include:
The goal of the surgery is to anatomically reconstruct the PCL, restoring the knee’s ability to prevent the shinbone from moving too far backward, thereby eliminating instability.
Understanding the recovery process helps set realistic expectations and maintain motivation throughout rehabilitation. Recovery duration varies based on injury severity and treatment approach. Both non-surgical and surgical treatments require patience and commitment to rehabilitation.
The timeline for recovery varies dramatically based on the injury grade and the chosen treatment path:
The long-term outlook for a successfully treated PCL injury is positive, but it relies heavily on sustained effort during rehabilitation. The focus remains on functional strength, specifically strengthening the quadriceps, which acts as a dynamic brace for the knee.

Dr Yong Ren brings extensive expertise to the field of minimally invasive orthopaedic procedures. His background includes specialist training in Switzerland, focusing on complex orthopaedic trauma and reconstruction, underscoring his capability in handling simple to highly complex joint issues.
Choosing us means you benefit from:
Dr Yong Ren’s practice prioritises the least invasive techniques, leading to smaller scars, less post-operative pain, and faster return to function.
We believe in treating the whole patient, not just the injury. This includes a full, multi-modal pathway from non-operative treatments (like physical therapy and injections) to the latest surgical techniques.
We provide clear, locally-relevant guidance on everything from the procedure itself to the intricacies of Medisave claimability and insurance processing in Singapore.
If you have been living with persistent pain, or if you have questions about your orthopaedic condition and wish to explore personalised, advanced treatment options, we encourage you to consult with Dr Yong Ren.
Take the first step toward a pain-free life with a $150 Knee Pain Consultation & X-ray.
